Immunotherapy of Benign Prostatic Hyperplasia (BPH) or Adenoma Prostate and Prostate Cancers
 What are BPH (Adenoma Prostate) and Prostate Cancers?
What are BPH (Adenoma Prostate) and Prostate Cancers?
BPH or Adenoma Prostate
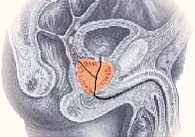
Prostate is a male sex gland, which secretes seminal fluid that combines with sperm to form the semen (nearly 95% of the seminal fluid consists of prostate fluid). In great number of adult men population we notice an enlargement of this gland due to the mutative changes in the prostate cells caused by various mutagenic (cancerogenic) agents. Below in Fig.1, the chromosomal sites with mutative changes in benign or malignant prostatic diseases are illustrated.

Fig. 1. Chromosomal map with notification of gene sites, where mutative changes had taken place in benign or malignant prostatic diseases
This enlargement of prostate gland is known as Benign Prostatic Hyperplasia (BPH) which causes various urinary problems depending on the stage of growth. If the enlargement involves mainly the glandular tissues, then it is called the adenoma prostates.
According to different sources, the BPH or adenoma prostate is present approximately in case of 20 % of the men at the age of 40 years, 70 % at the age of 60 and 90 % at the age of 80 years and above [1, 19, 37, 38]. As the growth is usually quite gradual, for the majority of men significant problems may not be perceptible but nearly one third of men will have problems for which they need to seek treatment. The early clinical problems may range from mild to moderate symptoms: weak or sluggish urinary stream, nycturia, increased urinary frequency, increased urinary urgency and impotence.
As the disease progresses, the adenoma prostate causes permanent changes in all parts of the urinary path; especially the upper urinary paths and kidneys get worsen. The increasing mass of the adenoma causes considerable elongation and compression of urethra and may result into severe cystectasia due to back flux of urine from urinary vessel into upper urinary paths, severe urination disorder (frequent and difficult), chronic urinary tract infections, renal insufficiency and acute dysuria which requires emergency catheterization of the urinary vessel. In case of a fast growth of the disease an urgent surgical interventions may be needed.
Among the prostate problems, BPH (adenoma prostate) and Prostatic Intraepithelial Neoplasia (PIN) are believed to be the most likely precursor of prostate cancer. PIN is a proliferative lesion i.e. it is composed of prostatic epithelial cells that are dividing more rapidly than normal epithelium. However, the cells have not yet become cancerous [22, 23].
Moreover, it is possible to have both BPH and prostate cancer at the same time.
Prostate Cancers
Prostate cancer is the most common cancer, excluding skin cancers, in American men. The American Cancer Society (ACS) estimates that during 2005 about 232,090 new cases of prostate cancer will be diagnosed in the United States. A little over 1.8 million men in the United States are survivors of prostate cancer. Prostate cancer is the second leading cause of cancer death in American men, exceeded only by lung cancer. The American Cancer Society estimates that 30,350 men in the United States will die of prostate cancer during 2005. Prostate cancer accounts for about 10% of cancer-related deaths in men [3]. One man in six will be diagnosed with prostate cancer during his lifetime. As in case of BPH or Adenoma Prostate the prostate cancers are also seen mostly after 40 years of age. But, unlike BPH in prostate cancer basically the prostate tissue is involved rather than the glandular structures. Because of this, cancer may develop in a normal, enlarged or operated prostate. Similarly, both cancer and adenoma may exist together in the same prostate.
In early stages, prostate cancer is an insidious disease, as it doesn't have specific symptoms. This is one of the main reasons for late diagnosis - at those stages when the cancer has invaded neighbouring tissues and organs (rectum, bladder base, urethra) leading to urethral and rectal bleedings, severe urinating disorders and so on. The distant metastases may cause a variety of symptoms depending on the invaded organ: severe bone pain and pathologic fractures, problems with blood cell production in advanced stages, respiratory problems, bleedings, liver and renal insufficiency are some of the lethal problems that may accompany advanced prostate cancer.

The conventional treatment options and their efficacies
In case of BHP or adenoma prostate
For earlier stages with minor or moderate symptoms: starting from "watchful waiting" approach to medications such as a-blockers and Finasteride, low invasive physiotherapy and surgical manipulations are available for treatments. Traditional treatments for prostate cancer, while common, can be expensive. Luckily many health insurance plans are beginning to cover newer techniques.
Watchful waiting involves periodic examinations - about once a year to see if the symptoms are progressing or not. This enables the doctors to decide with medicinal or surgical interventions on time.
The most successfully used medicines are hormone therapy - Finasteride (Proscar™) [16, 26, 27, 41]. In about fifty percent of men, the prostate will start to shrink, although this will take at least 6 months, while treatment usually lasts a few years, sometimes forever. The diminished prostate size results into improvement or complete disappearance of urinary problems.
Among a-blockers: Prazosin (Minipres™), Doxazosin (Cardura™), Terazosin (Hytrin™), Tamulosin (Flowmax™/Omnic™), Alfuzocin (Xatral™) are in use [25].
Although in most of the patients with BPH these medicines may improve the urinary flow, they do not stop the prostate growth. The other fact is that they need to be taken continuously to achieve necessary therapeutic effects and thus the side effects like dizziness, slight low blood pressure, erection problems are often seen.
Thermotherapy and laser therapy are the two most effective physiotherapies used in the treatments of BHP or adenoma prostate. Transurethral microwave thermotherapy (TUMT) uses special machines (Prostatron™, Targis™, Prostalund™) with catheter to deliver microwave energy (high temperatures) within the prostate which can destroy prostate cells locally, resulting into regression of the prostate size and improving urinary flow [24, 25, 28, 35, 36].
High-energy light beams-lasers can be applied as variety of low invasive surgical manipulations. Like thermotherapy, the high temperature induced by a laser beam vaporizes tissue masses. To localize the laser beam specifically to the prostate, modified cystoscope or transrectal ultrasound are used. The leading techniques for this therapy are: Visual Laser Ablation of the Prostate (VLAP) [30, 31]; Contact Laser, Interstitial Laser Coagulation; TransUrethral Laser-Induced Prostatectomy (TULIP) [32, 36]; holmium: YAG laser resection of the prostate (HoLRP) [34]. Laser prostatectomy is a less invasive alternative to transurethral resection of the prostate (TURP) and show promising successes in correcting BPH symptoms; but again due to involvements of high techniques, costs (for example - 10,000-12,000 USD for a single course of VLAP or TULIP are not unusual) and side effects like bladder irritation or permanent retrograde ejaculations, their use for common people are rather limited.
The surgical treatments are applied to release severe symptoms in late stages. Transurethral resection of the prostate (TURP) is the most successful and common treatment for BPH and thus is considered as "the gold standard" among these treatment options. The operation is done without external incision with the help of a special instrument called resectoscope and lasts for about 90 minutes. When the prostate is only slightly enlarged, a modified version so called transurethral incision of the prostate (TUIP) may be a better option. TUIP has less risk of complications (retrograde ejaculation, impotence, incontinence, bleeding) than TURP [25, 33, 36, 39, 40].
Another recent advancement is the use of prostatic stents. These are titanium/gold-like springs that are placed under direct vision through the penis into the prostate to hold the prostate apart and relieve the urinating problems. Main advantages: easy and quick method with relatively good effects. Drawbacks: displacements of the stent position, frequent irritative voiding symptoms following the procedure [25, 36].
When the prostate had grown to bigger sizes - Open Prostatectomy is performed. The overall result in terms of improvement of symptoms is much better and long lasting in comparison with other treatments, though it has higher obvious surgical risks. The remarkable drawbacks from these surgical treatments, beside the usual surgical risks, are retrograde ejaculation (resulting into a failure to father children) and possibilities of the disease and symptoms to come back over times.
In case of prostate cancers
The range of treatment options that are practiced today in prostate cancers, like in other types of cancers, involve from non-invasive methods - Watchful waiting, hormone therapy, chemotherapy, cryotherapy, radiotherapy to most radical operations.
Treatment of prostate cancer needs to be individualized. Decisions regarding treatment options are often based on the clinical stage and grade, gleason score [43, 44, 45] rate of prostate specific antigen (PSA) [42, 47, 48, 49, 51] rise as well as the patient's current clinical status – age, life expectancy, presence or absence of other concurrent significant medical problems and so on. The Partin coefficient tables – a combine data on the PSA value, the Gleason score, and the clinical stage was elaborated by a group of urologists at the Brady Institute for Urology at Johns Hopkins University (revised in May 1997). It can be used to predict pathological stage of localized prostate cancer which is very important in deciding how to treat a patient further.
Watchful waiting can be appropriate for patients whose cancer has been detected at a very early stage in whom the amount of cancer cells (size) is very small (as measured by PSA test and biopsy) and when the cancer is not highly aggressive (gleason score 6 or less). The main advantages of watchful waiting are avoidance of severe side effects of surgery, radiation, or hormonal treatments and avoidance of treatment-associated expenses. On the other hand patient carry an obvious risk of the cancer being developed beyond control before the doctor see the necessity to recommend any treatment interventions. The PIVOT (Prostatic Intervention versus Observation Trial) is still in progress and data will not be available for many years [53, 54, 55].
Hormonal therapy (androgen ablation therapy) though usually reserved for advanced prostate cancer, can be combined with the primary treatment plan (post-prostatectomy or with radiation therapy) as a supplementary therapy, especially where there is high risk of recurrences. In certain cases, for example where the cancer is more aggressive and surgery or radiation is not possible, it is used as a major therapy.
The efficiency of certain hormone therapy plus chemotherapy in treating prostate cancers is still under clinical studies [56, 58].
Chemotherapy is mostly only in case of hormone-refractory prostate cancer. The administration of Mitaxantrone plus prednisone, Estramustine (Emcyt) have showed more success than others in this case, although usual side effects - hair loss, leukopenia, anemia and nausea are common.
Cryotherapy (freeze therapy) or Cryosurgery [46] is one of the novel and the few potentially curative treatment approaches, which is being used in modern clinics today to treat initial or recurrent prostate cancers; basically after radiation therapy or seeds. It may be offered as an alternative to Brachytherapy (seeds), in patients who have urinary obstructive symptoms, as it helps to open the urinary channel over time. Long-term results are not yet available and the side effects like impotence and incontinence constrain its use within prescribed limits [46, 64, 65, 66].
Radiation therapy is the second major options to treat prostate cancer after surgery. Several different forms of radiation therapy: external beam, Conformal external-beam therapy, intensity-modulated radiotherapy, brachytherapy or radioactive seed implantation, together with several forms of combined therapy have been elaborated for the treatments of different stages of prostate cancers [55, 67, 65]. It being less invasive than surgery may stand as the first choice of treatments for those patients whom the surgery is of too big risk - for example older, or patient with other serious concurrent health problems. Now the highly precise and modulated new techniques for conformal dosed radiotherapy being available, this therapy is more and more used effectively even in younger patients.
However, radiotherapy far does not meet the demand of the current prostate cancer problems. For example, in high Gleason grade (8, 9 and 10) cancers, radiation therapy has poorer long-term results than surgical therapy. Radiotherapy is a locally targeted - treatment and thus, in case of metastatic prostates its value as a conventional therapy drastically falls. The more virtuous use of radiotherapy is as a palliative method in bone metastases to control local pain associated with skeletal prostate metastasis.
The other moment is, how much the radial beam may cannot be conformable and modulated, its impact on the neighboring tissues, organs and at last in the overall organism can be only minimized but can not be avoided completely. And thus the long-term harsh adverse effects - immune suppressing effects, leucopoenia, anemia, nausea has made it a limited and little dubious method for many prostate cancer patients.
As in other cancer cases, the best long-term cures are seen after surgical treatment for prostate cancer - radical prostatectomy. In terms of clinico-functional outcomes, there are two types of radical prostatectomy: nerve-sparing and non nerve-sparing. In general, the surgical methods are best approved in relatively younger patients with aggressive (stage T2 or Gleason score 7) & clinically localized prostate cancer. Moreover, the recent new techniques, modifications in prostate surgery such as seminal vesicle sparing or laparoscopic techniques have not only minimized the surgical complications (hazards of anesthesia, risk of blood loss, surgical intra- and post- operative mortality rates) and period of hospital stay but also have significantly improved the long-term cancer survival rate. Surgery is uncommonly done for patients age 70 and over, as the overall benefits do not outweigh the amount of risks involved. The disadvantages may include impotence, the inability to get or sustain an erection. Other postoperative problems may include incontinence, the inability to control urine after the surgery (may be temporary or permanent), loss of ejaculation and fertility etc. The surgical treatments for metastatic and androgen-independent PC are limited and rather unsatisfactory [28, 44, 50, 54].
The novel global approaches in prostate problems
The limited successes of the conventional methods of prostate treatments described above which have been practiced over many years on one hand, and the ever-growing global prostate cancer problems on the other hand, have urged the modern medicine to look for other alternatives which have more effective and etiological approaches to solve the existing prostate problems.
Angiostatic Approach to Cancer Therapy that chokes off the blood supply to prostate tumors is showing promising results.
Immunotherapy based on the molecular biology of Genetics and immunology is novel treatment option especially for advanced prostate cancers. During last decade hundreds of immunotherapeutic drugs and vaccines have been launched in different stages of clinical trials providing new hopes in the cancer world [10, 16].
And fortunately, 'the vast significance of the immunological aspects in the genesis and treatment of the malignant tumors including prostate cancers' is no more a subject of discussion as used to be few years ago.
The tumor-targeted immunological approaches can be divided into cytokine-based therapies, tumor-associated antigen-based therapies, tumor vaccines, and dendritic cell-based therapies.
Over a hundred drugs and vaccines for treating prostate cancer are currently in clinical trials - for example; or the cancer specific vaccines (like antitumor vaccine RESAN) that rev up the immune system to attack prostate tumors.
How can immunotherapy solve the global prostate problems?
Today it is absolutely clear that cancers are developed in those particular people who have weak general immune responses; and thus only the proper immunotherapy can re-establish this immunological reactivity in them to fight adequately against the cancer. The most important part in defeating cancer is a well working immune system...
The important components of an effective immune response have been elucidated in recent years. An understanding of the dysfunction of the immune response in cancer in one or more of these components has led to a variety of immunotherapeutic approaches. These therapeutic strategies are designed to stimulate dendritic cell proliferation, promote antigen uptake and processing, stimulate an effector cell response via direct antigen presentation, or target tumor cells via antibody therapy. Many approaches in prostate cancer have demonstrated successful induction of the desired immune response.
Among the hundreds of demonstrative scientific research works towards this field, here are some of the most authentic evidences.
Particularly the prostate, represents a unique site for immunotherapy because prostate-specific immunity can be generated without much efforts. Antibodies and cell-mediated immunity, induced by either active or passive immunization, represent potential means to target specifically prostate tumor cells [21].
Although local prostate cancer (PC) can be cured in most cases by radical prostatectomy, therapies for metastatic and androgen-independent PC are limited and rather unsatisfactory. In the field of passive immunotherapy, chimeric/recombinant antibodies and derivatives thereof show promising results in early clinical trials (phase I/II) [16].
Prostate-specific membrane antigen (PSMA) is a potential target in prostate cancer patients because it is very highly expressed and has been reported to be up regulated by androgen deprivation [17, 29].
PSA vaccine constructs are immunogenic and induce antibody responses to a multitude of surface antigens on prostate tumor cell lines by epitope or determinant spreading after stimulation of the immune system by PSA immunization [21, 29].
The immunological data were more encouraging, with several patients from each arm of the trial having an increase in cytokine production, increases in specific antibodies and evidence of T-cell proliferation in response to the vaccinations and suggests that further exploration of immunotherapy in less advanced disease may yield more encouraging clinical responses [20].
Many tumor-associated antigens represent tissue differentiation antigens that are poorly immunogenic. Their weak immunogenicity may be due to immune tolerance to self-antigen. Several research outcomes have demonstrated that xenoantigen immunization can break tolerance to a self-antigen in humans, resulting in a clinically significant antitumor effect [18].
The major interferences in the prostate cancer vaccines development
The major obstacles in the R&D of prostate cancer vaccines are:
generation of inadequate immune responses by the tumor-associated antigens, presence of vast number of prostate specific antigen epitopes (heterogenecity), involvement of several biochemical mechanisms in the generation of immune answers, absence of effective and reliable monitoring systems for the assessment of cancer vaccine efficacy as well as the incomprehensible world cancer vaccine development regulatory system (concerning the present urgency in finding the solution of prostate problems) and the huge financial barriers.
To know more about the current problems in the immunotherapy click here.
How can RESAN vaccine solve your prostate problems?
The antitumor vaccine RESAN beside the glycoprotein analogous to 22 peptide fragments of the telomerase ferment (hTRT), contains more than 40 different tumor specific antigen fragments (epitopes) (imitators) including imitators of certain prostate antigen epitopes (click here to see the full list of tumor antigens whose certain epitopes are imitated by RESAN vaccine).
Below in Fig.2 and Fig.3 are shown the amino acid sequence of two antigens of prostate cancer (the antigen fragments (epitopes) which are imitated by the vaccine RESAN are in bold-letters and underlined). Fig 4. is illustrated spatial PSA antigen structure.
Fig. 2. PROSTATE-SPECIFIC MEMBRANE ANTIGEN (PSMA). HUMAN
mwnllhetdsavatarrprwlcagalvlaggffllgflfgwfikssneatn itpkhnmkafldelkaenikkflhnftqiphlagteqnfqlakqiqsqwke fgldsvelahydvllsypnkthpnyisiinedgneifntslfeppppgyen vsdivppfsafspqgmpegdlvyvnyartedffklerdmkincsgkiviar ygkvfrgnkvknaqlagakgvilysdpadyfapgvksypdgwnlpgggvqr gnilnlngagdpltpgypaneyayrrgiaeavglpsipvhpigyydaqkll ekmggsappdsswrgslkvpynvgpgftgnfstqkvkmhihstnevtriyn vigtlrgavepdryvilgghrdswvfggidpqsgaavvheivrsfgtlkke gwrprrtilfaswdaeefgllgstewaeensrllqergvayinadssiegn ytlrvdctplmyslvhnltkelkspdegfegkslyeswtkkspspefsgmp risklgsgndfevffqrlgiasgrarytknwetnkfsgyplyhsvyetyel vekfydpmfkyhltvaqvrggmvfelansivlpfdcrdyavvlrkyadkiy sismkhpqemktysvsfdslfsavknfteiaskfserlqdfdksnpivlrm mndqlmflerafidplglpdrpfyrhviyapsshnkyagesfpgiydalfd ieskvdpskawgevkrqiyvaaftvqaaaetlseva
Fig. 3. PROSTATE SPECIFIC ANTIGEN PRECURSOR (PSA). HUMAN
mwvpvvfltlsvtwigaaplilsrivggwecekhsqpwqvlvasrgravcggv lvhpqwvltaahcirnksvillgrhslfhpedtgqvfqvshsfphplydmsll knrflrpgddsshdlmllrlsepaeltdavkvmdlptqepalgttcyasgwgs iepeefltpkklqcvdlhvisndvcaqvhpqkvtkfmlcagrwtggkstcsgd sggplvcngvlqgitswgsepcalperpslytkvvhyrkwikdtivanp
 Fig 4. PSA antigen structure. The yellow parts are the antigen fragments (epitopes) which are imitated by RESAN vaccine
Fig 4. PSA antigen structure. The yellow parts are the antigen fragments (epitopes) which are imitated by RESAN vaccine
In such unique combination of multiple tumor antigen epitope imitators, RESAN can trigger vigorous antitumor response against prostate tumors. Moreover, its glyco-structures play an important role in the augmentation of this immune response. This is the exact type of cancer vaccine the scientists of the world have been exploring over last decade. The vaccine is effective in treatment of BPH and in prostate cancer. When it is used rationally (click here to see the most rational use of RESAN) the results are very promising. In case of BPH or adenoma prostates, the elaborated immunotherapy can be used solely. Here a considerable regression in prostate size, normalization of PSA levels and tremendous improvements in clinical symptoms are observed within 4-6 weeks after the vaccination.
In case of prostate cancer, the better results are expected particularly when it is combined with surgical treatments - check or regress metastatic growths, destroy micrometastases and prevent relapses resulting a long- term remission. The results can be monitored tracing the decreasing levels of tumor markers (PSA levels), incresing levels of cytokines or shrinking tumor sizes in CT and ultrasound examinations.
In those cases when operations are impossible or of too big risks, RESAN can be an alternative treatment as an non invasive, non toxic and non destructive methods which works simply by improving patients self immune system sufficiently to release the clinical problems.
As mentioned above, prostate cancer may be developed on a background of BPH (adenoma prostate) and Prostatic Intraepithelial Neoplasia (PIN). Moreover, the adenoma prostate may disguise the initial period of the prostate cancer. In these cases the level of PSA may vary from 4 to10 ngm/mls. When the level of PSA is higher than 10 ngm/mls the diagnosis of the prostate cancer does not arouse much doubt. It is mainly when the level of PSA is in between 4 and 10 ngm/mls, many difficulties arise to make a right decision: whether it is an adenoma or the initial stage of prostate cancer (or progression of the diseases after radical treatments). On the other hand, namely when the level of PSA is in between 4 and 10 ngm/mls, the use of the vaccine is most effective to control/prevent the development of prostate cancer (Vaccination for the Prevention of Cancers), resulting into a complete normalization of PSA level (in 90 % of the patients) within 1-2 months after the introduction of the vaccine.
Because it possess no serious side effects and is practically safe for all stage tumor patients, RESAN can bring many benefits even in advanced cancer patients, patients in whom the traditional methods happen to be ineffective and in the patients who experience relapses after these treatments (A New Approach in the Treatment of Advanced Cancers).
 Fig. 5. The decrease in the PSA level after the vaccination
Fig. 5. The decrease in the PSA level after the vaccination
The Patient candidates for 'Watchful waiting' approach would also benefit from vaccine RESAN. For them, it can even be the first choice of treatment for it being a safe-treatment with real potential to result into an absolute cure.
Below, it is demonstrated the PSA level changes observed after vaccination by RESAN in the patients with prostate problems (based on clinical assessment of patients with prostate problems).
The overall efficacy of RESAN immunotherapy in BPH
The histological research studies of an adenoma have proved that it consists of glandular derivations, covered by a cylindrical epithelium; cystic cavities and fibres of a connective and muscle tissue. Depending on predominance of tissue type, 4 forms of BPH have been distinguished, on which depends the efficiency of an immunotherapy by RESAN vaccine.
1. Glandular (adenoma) - immunotherapy is effective
approximately in 80-85 % of cases.
2. Fibrotic (fibroadenoma) - the immunotherapy is
effective approximately in 80-85 % of cases.
3. Myomatous (adenomyoma) - the immunotherapy is
effective approximately in 50-60 % of cases.
4. The mixed form of a neoplasm - immunotherapy is
effective approximately in 60-85 of % of cases.
Note: The most common cases are the first two forms.
Conclusion:
The traditional conventional methods of treatment - particularly the radiotherapy, chemotherapy, hormonal therapy and the surgery have shown limited successes in solving the prostate problems. Besides, they possess unavoidable side effects which may do more harm to patients than help, especially to weak patients (practically as a rule, all cancer patients have weak immunological and clinical status).
The most successful treatment choice-surgery choice - surgery may cause unpleasant adverse effects. Because radical prostatectomy can result in severing nerves and blood vessels related to sexual or bladder function, it has high potential to make patients impotent, incontinent, or both.
Although local prostate cancers can be cured in most cases by radical prostatectomy, therapies for metastatic and androgen-independent PC are limited and rather unsatisfactory.
The second conventional prostate treatment method - radiation therapy is a treatment option that may be less traumatic than radical prostatectomy and appears to have similar results when used in early-stage patients. Radiation therapy also has adverse effects, including impotence in up to 40 to 50 percent of patients which make it a very limiting-use.
So, the prostate problems particularly prostate cancer remains a difficult clinical problem regardless of intensive scientific research works and billions of dollars spent every year in the research and development of novel therapy strategies for their effective control and treatment.
In past decade, immunology has demonstrated in the scientific world its huge potentials and competence for solving the cancer problems. And in particular, the immunologic approach of solving the tumor problems has proceeded most revolutionary in prostate direction; achieving many encouraging results. Though there are still many unsolved questions in cancer immunology, the time has come to make it available for public use; the amount of proofs that had been illustrating its range of effectiveness, safety ness and urgency already out way all the counter arguments.
RESAN vaccine is one of those successful modern immunologic research work outcomes, which possesses immense anticancer activities, particularly against prostate tumors. According to the SRE RESAN company's scientific and clinical research works outcomes - it is, without doubt, one of the most wide ranged and strongest novel cancer vaccine so far that can be used as a target for antigen-specific immunotherapy.
Unlike most of the other cancer types, prostate cancers grow quite slowly and it requires lifelong follow-up! Unfortunately, prostate cancer can recur many years after apparently successful treatment. This is why vaccines like RESAN together with the 'Routine screening system for prostate cancer' could play unique role in prophylaxis and treatments of prostate cancers to achieve a full control over the world prostate problems.
References:
1. Prostate Cancer. No One Answer for Testing or Treatment. John Henkel. FDA/Office of Public Affairs. Online.
2. MedNews Screening for prostate cancer. Digital Rectal Examination and Prostate Specific Antigen. NCI. Online.
3. What Are The Key Statistics About Prostate. 2005© American Cancer Society, Inc.
4. Natural anti-Gal antibody as a universal augmenter of autologous tumor vaccine immunogenicity. Immunology Today. vol.18, No. 6, june 1997, pp. 281-285. Uri Galili and Denise C. LaTempl.
5. Tumor antigens recognized by T cells. Immunology Today. vol.18, No. 6, june 1997, pp. 267-268. Thierry Boon, Pierre G. Coulie and Benoit Van den eyde.
6. Gene therapy of prostate cancer: current and future directions. Endocr Relat Cancer 2002 Jun;9(2):115-39. Mabjeesh NJ, Zhong H, Simons JW. Winship Cancer Institute, Department of Hematology and Oncology, Emory University School of Medicine, 1365 Clifton Road, Suite B4100, Atlanta, Georgia 30322, USA.
7. PATE, a gene expressed in prostate cancer, normal prostate, and testis, identified by a functional genomic approach. Proc Natl Acad Sci USA 2002 Mar 5;99(5):3058-63. Bera TK, Maitra R, Iavarone C, Salvatore G, Kumar V, Vincent JJ, Sathyanarayana BK, Duray P, Lee BK, Pastan I. Laboratory of Molecular Biology and Laboratory of Pathology, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD 20892, USA.
8. Heterogeneous expression of MAGE-A genes in occult disseminated tumor cells: a novel multimarker reverse transcription-polymerase chain reaction for diagnosis of micrometastatic disease. Cancer Res 2002 Jan 1;62(1):251-61. Kufer P, Zippelius A, Lutterbuse R, Mecklenburg I, Enzmann T, Montag A, Weckermann D, Passlick B, Prang N, Reichardt P, Dugas M, Kollermann MW, Pantel K, Riethmuller G. Institute of Immunology, University of Munich, 80336 Munich, Germany.
9. Analysis of endogenous peptides bound by soluble MHC class I molecules: a novel approach for identifying tumor-specific antigens. Eur J Immunol 2002 Jan;32(1):213-22. Barnea E, Beer I, Patoka R, Ziv T, Kessler O, Tzehoval E, Eisenbach L, Zavazava N, Admon A.The Smoler Protein Center, Department of Biology, Technion, Haifa, Israel.
10. The latest research on gene therapy for prostate cancer. Online.
11. TAP off-Tumors on. Immunology Today. vol.18, No. 6, june 1997, pp.292- 298. Immunology Today. Barbara Seliger, Marcus J. Maeurer and Soldano Ferrone.
12. Prostate specific antigen inhibits immune responses in vitro: a potential role in prostate cancer. J Urol 2002 Aug;168(2):741-7. Kennedy-Smith AG, McKenzie JL, Owen MC, Davidson PJ, Vuckovic S, Hart DN. Urology Department and Haematology Research Group, Christchurch Hospital and Molecular Pathology, Canterbury Health Laboratories, Christchurch, New Zealand.
13. Prostate stem cell antigen: Identification of immunogenic peptides and assessment of reactive CD8+T cells in prostate cancer patients. Int J Cancer 2002 Dec 1;102(4):390-7.
Kiessling A, Schmitz M, Stevanovic S, Weigle B, Holig K, Fussel M, Fussel S, Meye A, Wirth MP, Rieber EP. Institute of Immunology, Medical Faculty, Technical University of Dresden, Dresden, Germany.
14. Role of prostate stem cell antigen in prostate cancer research. Curr Opin Urol 2002 Sep;12(5):401-6. Jalkut MW, Reiter RE. Department of Urology, University of California - Los Angeles School of Medicine, Los Angeles, California, USA.
15. Immunotherapy for prostate cancer. Rini BI, Small EJ.University of California at San Francisco Comprehensive Cancer Center, 1600 Divisidero Street, 3rd floor, San Francisco, CA 94115, USA.
16. Proscar Online.
17. A unique folate hydrolase, prostate-specific membrane antigen (PSMA): a target for immunotherapy? Tasch J, Gong M, Sadelain M, Heston WD.Department of Urology, Memorial Hospital, Memorial Sloan-Kettering Cancer Center, New York, NY 10021, USA.
18. Dendritic cell-based xenoantigen vaccination for prostate cancer immunotherapy. Fong L, Brockstedt D, Benike C, Breen JK, Strang G, Ruegg CL, Engleman EG. Department of Pathology, Stanford University School of Medicine, Palo Alto, CA 94304, USA.
19. Screening for prostate cancer. Online.
20. Allogeneic whole-cell vaccine: a phase I/II study in men with hormone-refractory prostate cancer. Eaton JD, Perry MJ, Nicholson S, Guckian M, Russell N, Whelan M, Kirby RS. Division of Oncology, St George's Hospital Medical School, London, UK.
21. Evidence of determinant spreading in the antibody responses to prostate cell surface antigens in patients immunized with prostate-specific antigen. Clin Cancer Res 2002 Feb;8(2):368-73.
Cavacini LA, Duval M, Eder JP, Posner MR. Beth Israel Deaconess Medical Center, 21-27 Burlington Avenue, Room 556, Boston, MA 02215, USA.
22. Prostatic Intraepithelial Neoplasia. David G. Bostwick, MD, MBA, FCAP. Dharam ramani, MD, ECAP. 2001 Bostwick Laboratories. Online.
23. Prostatic intraepithelial neoplasia is a risk factor for adenocarcinoma. Predictive accuracy in needle biopsies. Journal of Urology 1995; 154:1295-99. Davidson D, Bostwick DG, Qian J, et al.
24. TransUrethral Microwave Thermotherapy Using the Prostatron™. A. Non-Surgical Breakthrough in BPH Treatment. Kankakee Urological Associates, LTD * Riverside Medical Center. Online.
25. UROlog, BPH treatment. Based on information from various sources. Online.
26. Effectiveness of Proscar in Treating Enlarged Prostates. Susan A. Steeves. University of Texas Southwestern Medical Center 25-Feb-98.
27. PROSCAR® (Finasteride). Tablets Patient Information about PROSCAR ® (Prahs-car). Online.
28. How Is Prostate Cancer Treated? Americal foundation for Urologic Disease. Online.
29. The latest research on immune therapy for prostate cancer. Prostate Cancer Information Centre. infoaging.org Online.
30. Laser ablation of the prostate in patients with benign prostatic hypertrophy. Costello AJ, Bowsher WG, Bolton DM, Braslis KG, Burt J. Br J U 1992; 69:603-8.
31. VISUAL LASER ABLATION OF THE PROSTATE (VLAP) WITH BARE FIBER IN CONJUNCTION WITH LASER BLADDER NECK INCISION IN THE TREATMENT OF PATIENTS WITH BENIGN PROSTATIC HYPERPLASIA (BPH). Ann Saudi Med 1997; 17(2):191-194. Hasan M. A. Farsi, FACS, FRCS(C); Hisham A. Mosli, FACS, FRCS(C); Mohammed F. Alzemaity, FACS, FRCS(C); Ahmed Bahnasy, MD, PhD.
32. Laser Prostatectomy for Benign Prostatic Hypertrophy. The Regence Group, Medical Policy. Revised/Effective Date: 01/08/2002. Online.
33. TUIP (transurethrale Inzision der Prostata) f?r BPH (benigne Prostatahyperplasie . Prostatitis. neu in 2001. Online.
34. Holmium:YAG Laser Resection of the Prostate Versus Visual LaserAblation of the Prostate and Transurethral Ultrasound-Guided Laser Induced Prostatectomy. A Retrospective Comparative Study. Journal of Endourology, Vol.5, Number 2, 152-156, Mar 1998. Kitagawa M, Furuse H, Fukuta K, Aso Y.
35. Minimally Invasive BPH Treatments , Laser Surgery BPH Treatment, Transurethral Microwave Thermotherapy (TUMT), Transurethral Needle Ablation (TUNA®). ©Ethicon Endo-Surgery, Inc. 2001, 2002. Online.
36. CORNELL Physicians, BPH, Surgical Treatments , Surgery; TURP and TUIP, Minimally Invasive Procedures: Laser prostatectomy, Transurethral thermotherapy, Transurethral needle ablation (TUNA), Prostatic stents, Transurethral electrovaporization. Online.
37. Benign prostatic hyperplasia. Victoria Kennedy, RN, A.D.A.M. editorial (11/14/2001). Department of Urology, New York-Presbyterian Hospital Columbia Campus, New York, NY. Online.
38. Prostate Cancer UK, BHP (Benign Prostatic Hyperplasia). Online.
39. Prostate Cancer UK, Transurethral Resection of the Prostate (TURP). Online.
40. Transurethral prostatectomy for benign prostatic hyperplasia. Online.
41. Proscar for the Treatment of Prostate Cancer? Mark Scholz M.D. Stephen Strum M.D. June, 1995. Prosate cancer Research Institute. Online.
42. Prostate Cancer UK, Prostate-Specific Antigen (PSA). Online.
43. Gleason Grade. Online.
44.Salvage radical prostatectomy for radiorecurrent prostate cancer: morbidity revisited. Vaidya A, Soloway MS. J Urol 2000;164:1998-2001. Online.
45. Understanding Gleason Grading, Prostate Cancer UK. Online.
46. Cryotherapy. Drs. Werner, Murdock & Francis; P.A. Greenbelt - Laurel - Bowie, Maryland. Online - UROLOGY ASSOCIATES.
47. PSA (prostate specific antigen). Online.
48. Prostate Specific Antigen - Cancer information on MedicineNet.com Online.
49. PSA RapidScreen Test. CRAIG MEDICAL DISTRIBUTION INC. Online.
50. Doctor's Guide Publishing Limited. Radical prostatectomy often results in impotence and urinary incontinence. Online.
51. Patient Information PSA (prostate-specific antigen) Screening for Prostate Cancer. Journal of Family Practice 1993;37(5):435-6. Hahn and Roberts.
52. Partin Tables. Online.
53. MARIN UROLOGY. Vernon E. Weldon, M.D., Harry Neuwirth, M.D., Patrick M. Bennett, M.D. Watchful Waiting. Online.
54. Family Practice Notebook, Radical Prostatectomy by Scott Moses, MD, last revised 9/29/2002. Online.
55. Treatment of Prostate Cancer: Radioactive Seed Implantation , (Brachytherapy). Duke K. Bahn, M.D. Department of Radiology, Crittenton Hospital, Rochester, MI (248) 652-5611 .
56. Hormone Therapy Plus Chemotherapy in Treating Patients With Prostate Cancer. ClinicalTrials.gov processed the record on 2002-12-08. Online.
57. Chemotherapy for Prostate Cancer. UPMC cancer centres. Online.
58. Prostate Cancer Hormone Therapy. Online.
59. PROSTATE CANCER Treatment: Advanced Systemic Disease. U-M Comprehensive Cancer Center. Online.
60. Chemotherapy Combination Promising for Advanced Prostate Cancer. Taxotere and Emcyt Phase II Report. New York, May 7, 2001 (PSA Rising).
61. Taxotere®/Estramustine/Prednisone: New Standard of Care for Hormone-Refractory Prostate Cancer? © CancerConsultants.com
62. CHEMOTHERAPY. Drs. E. David Crawford, Aubrey Pilgrim, Stephen Strum, Israel Barken, Bob Leibowitz and Contributions from Several Survivors.
63. Brachytherapy for Prostate Cancer - Recovery Complications, Medicines and Heart Concerns. © Thomas P. Doherty, December 22, 2000.
64. Prostate Cancer: Cryotherapy. Online.
65. Prostate Radioactive Seed Implantation. The Newest Alternative for Treating Early Prostate Cancer. Radiation Medical Group, Inc. Online.
66. Cryosurgery in the Treatment of Prostate Cancer. Duke K. Bahn, M.D. Department of Radiology, Crittenton Hospital, Rochester, MI (248) 652-5611.